The Issues
RISING MATERNAL MORTALITY AND POOR HEALTH OUTCOMES
The rate of mothers dying in childbirth or due to pregnancy-related causes continues to climb in the U.S. even while it declines in other high-income countries.
What’s even more staggering is that more than 60% of maternal deaths in the U.S. are preventable and unnecessary.
Pregnancy related deaths in the U.S.
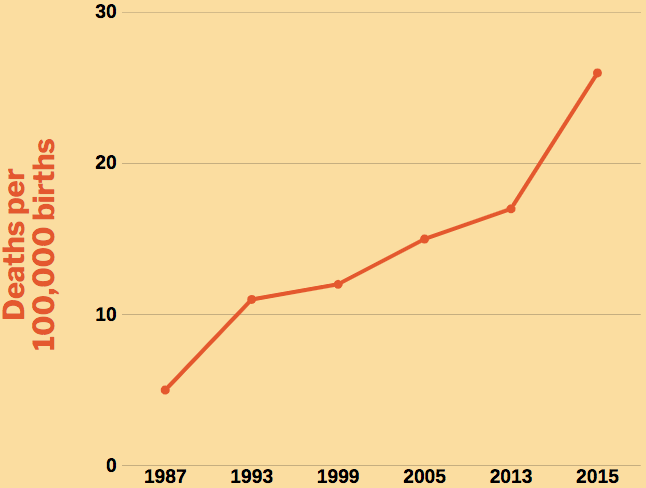
The figure above shows that the rate of maternal deaths quintupled in the last thirty years despite advances in maternal care.
WHY?
The reasons maternal death rates are on the rise in the U.S. include:
- Poor access to health care
- Racism, discrimination and disrespect
- Lack of integrated care models that address medical, behavioral and social needs comprehensively
- Misaligned incentives for health systems with maternal health outcomes
Because of these barriers, the U.S. has the highest rate of maternal death out of every high-income country.
It’s even worse for women of color. Maternal death for American Indian/Alaskan Native and non-Hispanic Black women is 3 to 4 times more likely to happen compared to white women.
But maternal mortality isn’t the only issue we care about. Keep reading to learn more about the issues facing women and families in the U.S.
Our mothers deserve better
The U.S. has the highest rate of mothers dying in pregnancy, childbirth, and within one year of giving birth than any other industrialized country. It continues to rise due to racial discrimination and a lack of access, information, and healthcare providers.
%
of pregnancy deaths
are preventable
1 in 6 women
Report feeling disrespected by healthcare providers during pregnancy

INTEGRATED MODELS OF CARE
Perinatal mood and anxiety disorders can appear during pregnancy, or days or up to a year after childbirth, and does not usually resolve without treatment. It is estimated that 15-21% of pregnant women experience moderate to severe symptoms of depression or anxiety. Without appropriate intervention, poor maternal mental health can have long term and adverse implications for mother, child, and family.
We need to improve access to integrated models of care for all persons throughout pregnancy, birth and postpartum periods.
March for Moms supports legislation and funding to ensure continuous access to health care coverage up to 1 year postpartum through Medicaid as well as private insurance reforms to protect families from gaps in coverage. Further, March for Moms supports legislation that promotes inter-professional collaboration with obstetricians, midwives, nurses, general practitioners, behavioral health providers, pediatricians and other medical professionals involved in the care of pregnant people.
An estimated
%
of PREGNANT WOMEN EXPERIENCE DEPRESSION OR ANXIETY AFTER CHILDBIRTH

Access to health care
There are major pockets of the US where individuals do not have access to needed maternity care services and/or do not have either Commercial or Medicaid insurance coverage.
Although many states are undertaking efforts to extend Medicaid coverage from the mandatory 60 days postpartum to 1 year postpartum, as see on the Figure.
March for Moms strongly supports Federal and State efforts to ensure that all birthing people have access to continuous insurance from conception up to one year postpartum.
State efforts in 2019 to extend Medicaid coverage for pregnant women beyond 60 days postpartum
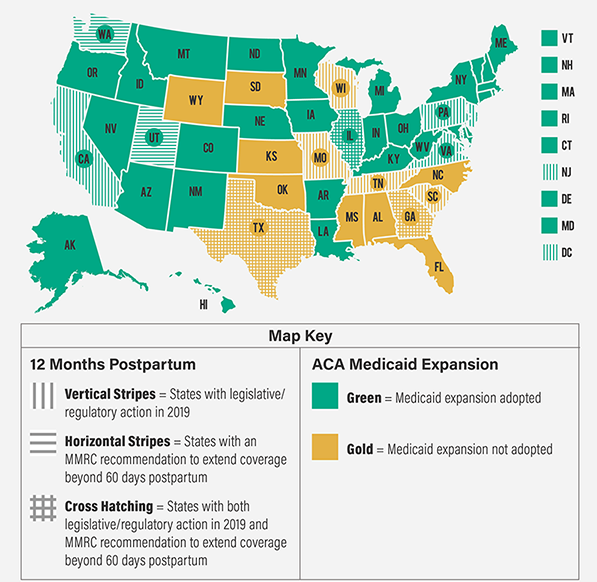
Source: Eckert, E, “It’s Past Time to Provide Continuous Medicaid Coverage For One Yea Postpartum,” Health Affairs Blog, Feburary 6, 2020. https://www.healthaffairs.org/do/10.1377/hblog20200203.639479/full/
Payment Reform
Today, the payment for maternity care by insurance companies is not aligned with accountability or outcomes for growing families. Total payment for a pregnancy and birth includes professional services paid to the individual clinicians who provide prenatal care, labor, birth and postpartum care as well as a facility fee paid to the hospital or birthing facility for the birth or cesarean, if applicable. Some payers group together these fees under a “global maternity fee,” which is paid to both the individual clinicians and the facility together.
This payment structure is deeply flawed as it does not cover high-value services such as group visits and doula care; it does not hold hospitals, facilities and clinicians accountable for the mother’s outcomes; and it does not encourage coordination between providers including behavioral health providers, primary care and pediatrics for the optimal health of the mom and the baby.
March for Moms supports the use of health care payment models that reward accountability for and models of care that demonstrate superior outcomes such as midwifery care, integrated team-based care, care in freestanding birth centers, and support from doulas. March for Moms supports ensuring that levels of payment for maternity and newborn care across birth settings are adequate to support access to a range of maternity care options across the nation.
Average Out-Of-Pocket cost of a birth in the United States

Health care disparities
Black and Indigenous birthing people are 2.5-4 times more likely to experience maternal mortality than white people. These preventable deaths occur each year as a result of racial and ethnic health disparities, which stem from systemic inequities including lack of access to care and pervasive racism. Approximately 83,000 preventable deaths occur each year as a result of racial and ethnic health disparities, including high infant mortality rates.
Further reading
Amnesty International. Deadly Delivery the Maternal Health Care Crisis in the USA: One Year Update
http://www.amnestyusa.org/sites/default/files/deadlydeliveryoneyear.pdf
CDC Maternal and Infant Health
https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pmss.html
CDC Premature Birth
https://www.cdc.gov/reproductivehealth/maternalinfanthealth/pretermbirth.htm
March of Dimes Premature Birth Report Card
http://www.marchofdimes.org/mission/prematurity-reportcard.aspx
Institute for Women’s Policy Research
https://iwpr.org/publications/paid-parental-leave-in-the-united-states-what-the-data-tell-us-about-access-usage-and-economic-and-health-benefits/
Bureau of Labor Statistics
https://www.bls.gov/OES/current/oes291161.htm
Bureau of Labor Statistics
https://www.bls.gov/oes/current/oes291064.htm
Think Progress
https://thinkprogress.org/how-the-zero-weeks-of-paid-maternity-leave-in-the-u-s-compare-globally-a8ba7f36f85b#.ocxvqtpvt
ASTHO Issue Brief
http://www.astho.org/Programs/Health-Equity/Maternal-and-Infant-Disparities-Issue-Brief/
CDC: Health United States 2015: With Special Feature on Racial and Ethnic Health Disparities
https://www.cdc.gov/nchs/data/hus/hus15.pdf
MomsRising.org: Raising Our Voices For Maternal Health
https://s3.amazonaws.com/s3.momsrising.org/images/Maternal__Health_Justice_Birth_Story_Book_Feb_2018.pdf
SOCIETY FOR MATERNAL FETAL MEDICINE
http://www.choosingwisely.org/societies/society-for-maternal-fetal-medicine/
ACNM Talking Points
http://www.midwife.org/acnm/files/ccLibraryFiles/Filename/000000004024/HR4385TPs.pdf